




ESI Group validates the proficiency of Rensair’s clean air delivery

Airflow is critical to the effective performance of portable air purifiers and an (often hidden) point of difference between competing brands. Successfully cleaning all the air within a room is a real engineering challenge. Many air purifier vendors make unsubstantiated claims. Some do little more than repeatedly clean the air around the unit itself, failing to mitigate the risk of infection from pathogens and leaving unsuspecting customers unprotected. Buyers should always seek corroboration of performance claims from independent tests undertaken by respected scientific laboratories and third party testing entities.
In Q1 2022, Rensair commissioned ESI Group to conduct thorough tests on the all-important airflow of the Rensair hospital-grade HEPA/UVC portable air purifier. ESI Group is a pioneer and world leader in predictive physics modelling and virtual prototyping. Established in 1973 and headquartered in France, the company’s prime service is to simulate product behaviour during testing and to evaluate the environment’s impact on product performance.
ESI’s study comprised both Computational Fluid Dynamics testing (Part 1) and in-situ modelling in a Birmingham hospital dental treatment room (Part 2)).
Part 1: Characterisation of flow through the unit
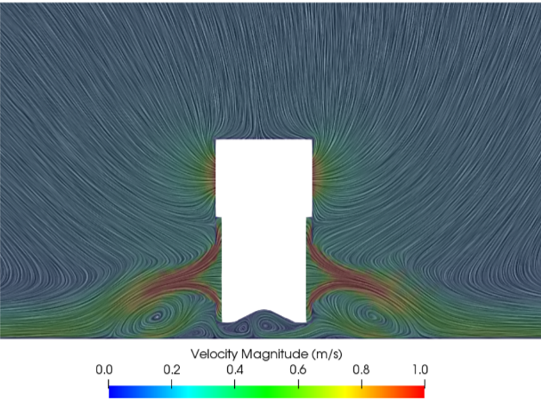
After confirming that the airflow rate on high and low settings was actually commensurate with the manufacturer’s claims (560 and 300 m3/h respectively), ESI conducted various tests on the direction and uniformity of the intake of dirty air and outflow of clean air. The tests reported hemispherical intake of dirty air from above and around the circumference of the unit, sucking in at 360 degrees regardless of the angle of the unit. Uniform pressure and velocity were recorded inside the filter drum, with no air escaping back up through the unit. The downward pressure forces air through the HEPA filter evenly, avoiding premature wear.

The tests also demonstrated an even distribution of outflowing air. This resulted in the conclusion that the Rensair device provides circumferentially and axially uniform clean air delivery at the lowest (300m3/h) and highest flow rates (560m3/h).

The next phase of testing analysed the outflow from the lower part of the unit and the subsequent clean air distribution throughout the room. The unit quickly spreads purified air at 360 degrees in a uniform, outward ‘radial jet’ motion parallel with the floor. This enhances room penetration and encourages toroidal circulation of airflow throughout the space, such that clean air bounces off the walls, then the ceiling and then back into the entire room. Importantly, the toroidal flow pressures particles and aerosols downwards, a key benefit during AGPs.
Part 2: Dental Treatment Room – Birmingham Hospital
The in-situ modelling comprised a large dental treatment room (44.7m3, compared to a typical dental practice room at circa 30m3) with three occupants and an integrated ventilation system delivering 5 air changes per hour (ACH), which under current UK guidance would require the maximum fallow period of 30 minutes.
On the high fan speed setting, which is generally recommended during AGPs, and with the Rensair unit supplementing the existing 5 ACH ventilation, the average age of air in the room stabilised at 158 seconds, with an air change rate of 17.6 and circulation efficiency of 65%. ESI concluded that “When used in isolation, or with the treatment room’s mechanical ventilation notionally turned on, the air circulation efficiency scales with ACH irrespective of installation location; and rates well in comparison with other commercial portable and wall-mounted units of similar capacity.”

Clearance – defined as a 99% reduction (log 2 reduction) of particles emanating from the patient – was logged at just 0.84 of a minute when combined with the existing 5 ACH. With the ventilation system turned off, the Rensair unit alone achieved clearance in 1.3 minutes on the high setting, with an ACH of 12.6. Evidence that a Rensair unit on its own can achieve 99% reduction in 1.3 minutes gives confidence that only the minimal fallow time is required between patients, thereby allowing pre-pandemic ways of operating and maximising patient throughput. Healthcare professionals should be encouraged to seek such validated performance data when comparing air purifiers.

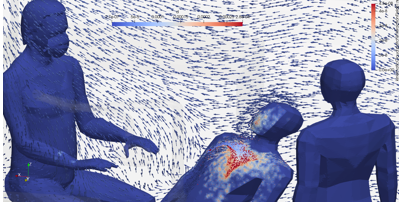
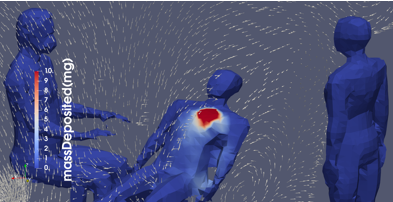
Of critical importance is that deposition and near patient flow field tests demonstrated high-to-low particle precipitation, drawing aerosols downwards from the AGP source and away from the dentist’s head, thereby providing protection from infectious particles. This occurred irrespective of the position of the Rensair unit in the room.
Conclusion and key findings
Key findings are:
- Rensair device stimulates a ventilation pattern corresponding to TOROIDAL.
- Rensair device in-situ demonstrates precipitation of aerosols from AGPs.
- Rensair device demonstrates a stable floor-wise room penetration, avoiding ground particulates (dust/carpet) ingestion into the device which may prematurely block the filter.
- Rensair device achieves rapid post AGP clearance ie. 99% reduction (log 2 reduction) of particles emanating from the patient.
Airflow is critical to the effective performance of air purifiers, regardless of the technology used to trap and/or inactivate pathogens. To successfully clean all the air in a room requires a combination of quality components (e.g. strong fan) and smart engineering (e.g. not creating exhaling drafts). Given the health risks at stake, manufacturers’ claims should not be taken at face value, but supported by 3rd party independent tests that show whether a unit is truly capable of cleaning all the air in a room, and in a decent sized room (rather than a small test chamber).
The ESI Group study unequivocally proves the efficacy of Rensair’s air purifier. Rensair’s robust centrifugal fan creates high, uniform static pressure in the cylinder and forces air effectively out through the dense HEPA filter, travelling across the floor and enhancing the penetration of clean air throughout the entire space.